Volume: 3 Issue: 2
The Goldilocks Zone in Advanced Neurorehabilitation: A Scoping Review on Optimal Challenge in Stroke Recovery
Year: 2026, Page: 38-49, Doi: https://doi.org/10.71325/ajjms.v3i2.26.14
Received: March 8, 2026 Accepted: April 8, 2026 Published: July 2, 2026
Abstract
Background: Stroke is a leading cause of long-term motor disability worldwide, affecting approximately 80% of survivors. Neurorehabilitation aims to harness neuroplasticity to restore motor function; however, determining the optimal level of task difficulty to maximise motor learning remains a critical clinical challenge. The "Goldilocks Zone" where task difficulty is neither too easy nor too demanding but appropriately calibrated to individual capability has emerged as a guiding concept in stroke rehabilitation. Objective: This scoping review aimed to map evidence on the theoretical foundations, clinical applications, and implementation of optimal challenge principles across diverse stroke neurorehabilitation interventions. Methods: A scoping review was conducted following the Arksey and O'Malley framework and reported in accordance with PRISMA-ScR guidelines. Eight electronic databases were systematically searched, supplemented by grey literature. Studies involving adults with confirmed stroke diagnosis that examined optimal challenge, adaptive difficulty, or related constructs within motor rehabilitation were eligible. A total of 242 records were identified; after duplicate removal and screening, 12 studies met all inclusion criteria and were included in the final synthesis. Results: Preliminary evidence suggests that adaptive difficulty adjustment may support superior motor learning and functional outcomes compared to fixed-difficulty approaches. The optimal challenge zone appears to correspond to success rates of 60-80%, with 70% emerging as the most commonly implemented target. Effective implementation suggests multi-dimensional difficulty adjustment, continuous performance monitoring and individualised calibration. Conclusion: Optimal challenge the Goldilocks Zone represents a theoretically well-grounded and clinically promising concepts for supporting neuroplasticity and functional recovery after stroke. Systematic investigations and cautious adoption of adaptive difficulty principles, enabled by advancing rehabilitation technologies, may represents a meaningful step toward personalised neurorehabilitation. Large-scale randomised controlled trials and long-term follow-up studies are warranted to consolidate the evidence base.
Keywords: Stroke rehabilitation; Optimal challenge; Goldilocks Zone; Challenge Point Framework; Adaptive difficulty; Neuroplasticity; Motor learning; Robot-assisted therapy; Virtual reality; Scoping review
INTRODUCTION
Stroke remains a leading cause of long-term disability worldwide, with motor impairments affecting approximately 80% of survivors and significantly limiting independence in activities of daily living[1, 2]. Neurorehabilitation aims to harness neuroplasticity, the brain’s capacity to reorganize and form new neural connections to restore motor function following stroke[3, 4]. However, a critical challenge in rehabilitation practice is determining the optimal level of task difficulty to maximize motor learning and functional recovery[5]. Tasks that are too easy fail to drive neuroplastic changes, while tasks that are too difficult can lead to frustration, learned non-use and maladaptive compensatory strategies[6-8].
The concepts of the “Goldilocks Zone,” representing conditions that are neither excessively demanding nor insufficiently challenging but optimally calibrated, has emerged as a guiding principle in neurorehabilitation. Applied to stroke rehabilitation, this concept proposes that task difficulty should be precisely matched to the individual’s current capability, thereby promoting engagement, motivation and effective motor learning[5, 9, 10]. The theoretical foundation for this concept is rooted in motor learning science, particularly the challenge point framework, which posits that learning is maximized when task difficulty is optimally balanced with learner’s skill level[11].
Recent technological advances in robot-assisted therapy, virtual reality, wearable sensors, and adaptive algorithms have enabled the systematic investigation and implementation of optimal challenge principles in stroke rehabilitation[12-15]. These technologies provide objective performance measurement, real-time feedback and automated difficulty adjustment, offering unprecedented opportunities to personalize rehabilitation and maintain patients within their Goldilocks Zone throughout recovery.
Despite growing interest in optimal challenge as a rehabilitation principle, the evidence base remains fragmented across modalities and lacks synthesis. The present scoping review therefore aims to: (1) map the theoretical frameworks underpinning the Goldilocks Zone concept in stroke rehabilitation; (2) characterise how optimal challenge principles are operationalised across diverse intervention modalities; (3) examine preliminary evidence comparing adaptive to fixed-difficulty approaches; and (4) identify gaps and directions for future research to advance evidence-based, personalised rehabilitation practice.
BACKGROUND AND THEORETICAL FOUNDATIONS
The Goldilocks Principle in Motor Learning: It postulates that optimal skill acquisition occurs when task difficulty is appropriately matched to the learner’s current ability level. This concept is grounded in decades of motor learning research demonstrating that learning is neither a simple function of practice quantity nor task difficulty alone but rather emerges from the interaction between task demands and learner capabilities. When tasks are too easy relative to skill level, they fail to provide sufficient challenge to drive neuroplastic changes and skill refinement. Conversely, when tasks exceed current capabilities, learners experience repeated failure, which can lead to disengagement, frustration, and the development of compensatory strategies that may hinder long-term recovery[4, 16, 17].
The optimal challenge zone refereed to here as the Goldilocks Zone represents a region of task difficulty that is insufficiently demanding to promote motor learning and neuroplasticity, yet sufficiently achievable to maintain engagement and permit successful performance across the majority of trials. This equilibrium is particularly relevant in stroke rehabilitation, where patients present with heterogeneous impairment profiles, variable rates of recovery and differing motivational characteristics. The Goldilocks principle therefore highlights the necessity of individualised, dynamic adjustment of task difficulty throughout the rehabilitation continuum[5, 18, 19].
Challenge Point Framework (CPF): Developed by Guadagnoli and Lee, provides the primary theoretical foundation for understanding optimal challenge in motor learning. The CPF proposes that the optimal challenge point for learning is determined by the interaction between task difficulty (functional task difficulty) and the performer’s skill level (nominal task difficulty). According to this framework, learning is maximized when the challenge point, the amount of interpretive and elaborative processing required is optimally matched to the learner’s current capabilities.
Several studies in this review explicitly applied the CPF to stroke rehabilitation. Lotay et al., (2019) implemented CPF based exercise scheduling in a mobile gaming device for hemiplegic stroke patients, demonstrating that adaptive scheduling based on CPF principles produced faster learning compared to fixed scheduling[20]. The study found that patients training with CPF based adaptation performed better than those with fixed conditions, though this effect was not observed in healthy volunteers performing near ceiling, suggesting that optimal challenge is particularly critical for individuals with impairments. Pollock et al., (2014) used the CPF to guide motor learning of stepping reactions for improved balance control in stroke survivors, providing a case series demonstrating the framework’s applicability to balance and gait training[21, 22].
The CPF emphasizes that optimal challenge is not static but must be continuously adjusted as skill develops. This dynamic nature of the challenge point has important implications for rehabilitation technology design, necessitating systems capable of real-time performance assessment and automated difficulty adjustment. The framework also highlights the importance of contextual interference, the practice schedule variability that enhances long-term retention, which can be integrated with optimal challenge principles to maximize learning efficiency[5, 18, 23, 24].
Neuroplasticity and Skill Acquisition: The neurological basis for optimal challenge in stroke rehabilitation lies in activity-dependent neuroplasticity, the principle that neural reorganization is driven by specific patterns of neural activity associated with behavioural practice. Neuroplasticity research has established several key principles relevant to the Goldilocks zone concept. First, neuroplastic changes are use dependent: neural circuits that are repeatedly activated are strengthened, while unused circuits may weaken. Second plasticity is experience specific: the nature of the practice task shapes the pattern of neural reorganization. Third, plasticity requires sufficient intensity and repetition: minimal practice doses fail to induce lasting neural changes[25, 26].
Critically, research suggests that neuroplasticity is maximized when practice occurs at an optimal level of difficulty. Tasks that are too easy may not provide sufficient neural activation to drive plasticity, while tasks that are too difficult may activate compensatory neural networks rather than promoting recovery of normal movement patterns. Smith et al., (2016) reviewed the implications of plasticity research for physiotherapy, emphasizing that task-oriented training must provide appropriate challenge and motivation to drive motor recovery. The authors noted that rehabilitation should progressively increase task difficulty as patients improve, maintaining an optimal challenge level throughout recovery[27-29].
Ballester et al., (2022) proposed a model of “virtuous and vicious cycles” in arm use and function post-stroke, suggesting that if arm use is raised above an effective threshold through appropriately challenging practice, patients enter a virtuous cycle where arm use and function reinforce each other via self-practice[29]. Conversely, if challenge is insufficient to promote arm use above this threshold, patients may enter a vicious cycle of declining use and function. This model underscores the importance of maintaining optimal challenge to promote sustained engagement and functional recovery[30, 31].
The neuroplasticity literature also highlights the importance of feedback and reward in driving learning. Optimal challenge is inherently motivating because it provides frequent enough success to activate reward circuits while maintaining sufficient difficulty to sustain engagement. This motivational aspect is particularly important in stroke rehabilitation, where maintaining patient engagement over extended practice periods is a significant clinical challenge[7, 18].
METHODS AND APPROACHES IN THE LITERATURE
This review is designed as a coping review following the PRSIMA extension for Scoping Reviews (PRISMA-ScR) framework, selected to map the breadth of evidence on optimal challenge in stroke rehabilitation across diverse intervention modalities, identify key concepts and highlight gaps for future research. This review does not aim to synthesise evidence to answer a specific clinical question (as in systematic review), but rather to characterise the extent, range and nature of available evidence [Fig. 1].
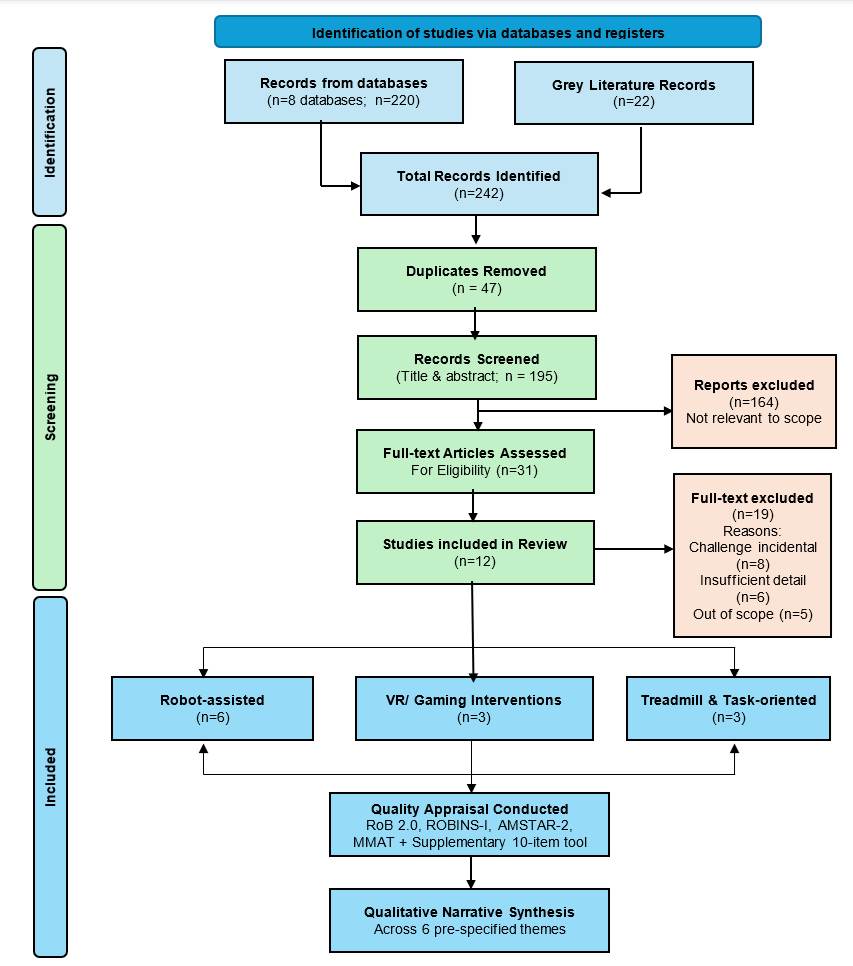
Fig. 1: Prisma-ScR flow Diagram
A systematic search was conducted across eight electronic databases: MEDLINE, EMBASE, CINAHL, Cochrane Library, IEEE Xplore, PsycINFO, Scopus, and Web of Science, supplemented by grey literature searching (Google Scholar, ProQuest, citation tracking). Search terms were organised into three Boolean blocks combining population terms (“stroke”, “cerebrovascular accident”, “hemiplegia”), intervention and concept terms (“optimal challenge”, “adaptive difficulty”, “challenge point framework”, “dynamic difficulty adjustment”, “Goldilocks Zone”), and modality terms (“robot-assisted therapy”, “virtual reality”, “treadmill training”, “task-oriented training”), with no date restriction applied.
Studies were eligible if they included adults with confirmed stroke diagnosis, addressed motor rehabilitation, and examined optimal challenge, adaptive difficulty, or related constructs (e.g., Challenge Point Framework, dynamic difficulty adjustment). All study designs were eligible. Two independent reviewers screened titles and abstracts, followed by full-text review; disagreements were resolved by consensus. Data were extracted using a standardised form capturing study design, population characteristics, intervention details, difficulty adaptation mechanisms, outcomes, and theoretical frameworks.
Quality appraisal was conducted descriptively using design-appropriate tools: Cochrane RoB 2.0 for RCTs, ROBINS-I for non-randomised studies, AMSTAR-2 for systematic reviews, and MMAT for conference papers and theses [Table. 3]. A ten-item supplementary quality scoring framework (maximum 20 points) was additionally applied across all included studies; this supplementary tool was selected because no single validated appraisal instrument covers the full heterogeneity of study designs included (empirical trials, theoretical reviews, theses and conference papers), and its use alongside design-specific tools allowed consistent quality grading [Table. 2]. Given substantial methodological heterogeneity, findings were synthesised using qualitative narrative synthesis organised around pre-specified themes: theoretical frameworks, mechanisms of difficulty adaptation, adaptive versus fixed difficulty evidence, optimal success rate targets, outcomes across impairment levels, and clinical implementation considerations. Of 242 records identified, duplicates were removed and title/abstract screening excluded papers not addressing stroke motor rehabilitation or not examining optimal challenge as a primary construct. Full-text review of 31 potentially eligible papers was conducted; further exclusions were applied where studies addressed challenge incidentally, lacked sufficient methodological details or fell outside the pre-specified scope. Twelve studies met all inclusion criteria and were included in the final synthesis.
Robot-Assisted Adaptive Training: It has emerged as a prominent platform for implementing optimal challenge principles in stroke rehabilitation, offering precise control over task parameters, objective performance measurement and automated difficulty adjustment. Multiple studies in this review developed and evaluated adaptive robotic systems designed to maintain patients within their optimal challenge zone.
Metzger et al., (2014) showed that an adaptive robot-assisted therapy system maintaining performance around a 70% success target was feasible and well-received by stroke patients[32]. while the pilot study did not include a fixed-difficulty control group, the successful maintenance of performance within the target range and positive patient feedback supported the adaptive approach. Zimmerli et al., (2014) validated a mechanism to balance exercise difficulty in robot-assisted rehabilitation, demonstrating that adaptive difficulty successfully maintained performance within target ranges and was associated with motor improvements[33].
Grimm et al., (2016) implemented closed-loop task difficulty adaptation during virtual reality reach-to-grasp training assisted with an exoskeleton for stroke rehabilitation[34]. Their system used real-time performance metrics to dynamically adjust task parameters, demonstrating that adaptive difficulty maintained patient engagement and promoted motor learning. Wang et al., (2022) developed a comprehensive control framework for adaptation of both training task difficulty and robotic assistance, implementing a computational model that optimized the balance between challenge and support to promote motor learning[35].
Several studies focused on specific aspects of difficulty adaptation in robotic therapy. Basteris et al., (2015) developed a lag-lead based assessment and adaptation of exercise speed for stroke survivors, using temporal performance metrics to adjust movement speed requirements and maintain optimal challenge[36]. Pan et al., (2019) conducted an experimental study on upper-limb rehabilitation training based on adaptive task levels, demonstrating that adaptive difficulty adjustment improved motor outcomes compared to fixed difficulty[37]. Giang et al., (2020) developed a motor improvement estimation and task adaptation system for personalized robot-aided therapy, implementing algorithms that predicted patient improvement trajectories and adjusted difficulty accordingly[38].
The robotic therapy literature demonstrates several common principles for implementing optimal challenge: (1) initial difficulty calibration based on comprehensive assessment, (2) continuous performance monitoring using objective metrics, (3) automated difficulty adjustment algorithms targeting specific success rates or performance thresholds, (4) concurrent modulation of task difficulty and robotic assistance, and (5) progressive reduction of assistance as patients improves. These systems typically adjust multiple task parameters including movement speed, workspace size, target accuracy requirements, and the degree of robotic guidance or resistance.
Virtual Reality (VR) and Gaming Interventions: VR and gaming technologies provide flexible platforms for implementing adaptive difficulty in stroke rehabilitation, offering engaging, motivating environments with precise control over task parameters and immediate performance feedback. Several studies in this review developed and evaluated VR-based interventions incorporating optimal challenge principles.
Rubino et al., (2024) investigated gamified practice for improving paretic arm motor behavior in stroke survivors, demonstrating that game-based interventions with adaptive difficulty improved motor outcomes[39]. The study emphasized the importance of balancing challenge and skill to maintain engagement and promote learning. Fridman D (2021) designed a game for upper limb rehabilitation following stroke that incorporated adaptive gameplay to balance physical and cognitive challenge with patient skill level[40]. The design process emphasized the importance of providing appropriate challenge, feedback, and progression to facilitate motor learning and maintain motivation.
Lobo P H (2024) developed a dynamic difficulty adjustment framework for serious games applications in neurorehabilitation, providing a systematic approach to implementing adaptive challenge in game-based rehabilitation[41]. The framework emphasized the need for real-time performance assessment and automated difficulty scaling to maintain patients within their optimal learning zone. Li et al., (2025) developed an online regulation system for task difficulty based on neuro- and motor-feedback to improve engagement in visual-motor tasks, demonstrating that adaptive difficulty based on physiological and performance metrics enhanced patient engagement[42].
VR and gaming interventions typically implement difficulty adaptation through multiple mechanisms including: (1) adjusting target size, speed, or trajectory complexity, (2) modulating the number of distractors or obstacles, (3) varying the time constraints for task completion, (4) scaling the cognitive demands of dual-task paradigms, and (5) providing adaptive feedback and scaffolding. These systems often incorporate game design principles such as progressive level structures, achievement systems, and narrative elements to enhance motivation and engagement while maintaining optimal challenge.
The gaming literature emphasizes the importance of the "flow state" a psychological state of optimal engagement that occurs when challenge and skill are appropriately balanced. This concept aligns closely with the Goldilocks Zone principle and highlights the motivational benefits of maintaining optimal challenge. Several studies noted that adaptive difficulty not only improved motor learning outcomes but also enhanced patient engagement, adherence, and satisfaction with rehabilitation.
Treadmill and Gait Training: Treadmill training represents an important application domain for optimal challenge principles in stroke rehabilitation, with several studies examining how challenge level influences gait recovery outcomes. Olsen et al., (2023) conducted a systematic review and meta-analysis examining whether challenge level contributes to the efficacy of treadmill interventions after stroke. The review analysed 23 studies and found that higher challenge levels operationalized through factors such as faster speeds, incline, dual-task conditions, or reduced body weight support were associated with greater improvements in gait speed and walking capacity. The meta-analysis provided quantitative evidence that challenge level is a critical determinant of treadmill training efficacy, with effect sizes increasing as challenge increased within the feasible range for patients[43].
Forrester et al., (2011) evaluated ankle training with a robotic device for improving hemiparetic gait after stroke, implementing adaptive difficulty adjustment based on patient performance. The study demonstrated that robot-assisted ankle training with appropriate challenge levels improved gait parameters including speed, symmetry, and ankle kinematics. The adaptive system adjusted the difficulty of ankle movement tasks to maintain patients within their optimal performance range, promoting motor learning while preventing excessive frustration or fatigue[44].
The treadmill training literature highlights several mechanisms for implementing optimal challenge in gait rehabilitation: (1) progressive increases in walking speed as patients improve, (2) gradual reduction of body weight support to increase the challenge of maintaining balance and propulsion, (3) introduction of incline or decline walking to vary task demands, (4) incorporation of dual-task paradigms that add cognitive or motor challenges, and (5) use of perturbations or obstacles to challenge balance and adaptability. These approaches share the common principle of systematically increasing task demands in response to patient improvement, maintaining an appropriate level of challenge throughout rehabilitation.
An important consideration in gait training is the balance between challenge and safety. Unlike upper extremity training where errors have minimal consequences, gait training involves fall risk that must be carefully managed. Adaptive treadmill systems typically incorporate safety features such as body weight support harnesses while still providing sufficient challenge to drive learning. The optimal challenge in gait training must therefore consider not only motor learning principles but also safety constraints and patient confidence.
Task Oriented Practice: Rehabilitation focused on practicing functional tasks relevant to daily living represents a foundational approach in stroke rehabilitation that inherently incorporates optimal challenge principles. Several studies in this review examined how optimal challenge is implemented in task-oriented training paradigms.
Woodbury et al., (2016) conducted a proof-of-concept study demonstrating that matching task difficulty to patient ability during task practice improves upper extremity motor skill after stroke. The study implemented a systematic approach to difficulty matching, adjusting task parameters such as object size, weight, and placement to maintain appropriate challenge for each patient's ability level. Results showed that patients receiving difficulty-matched training demonstrated greater improvements in motor skill compared to standard practice, providing direct evidence for the importance of optimal challenge in task-oriented training[45].
Platz et al., (2018) reviewed Arm Ability Training (AAT), a task-oriented approach that promotes dexterity recovery through systematic practice of functional tasks with progressive difficulty. The AAT approach emphasizes the importance of selecting tasks that are challenging yet achievable, providing clear performance criteria, and systematically progressing difficulty as patients improve. The review highlighted the neurobiological basis for AAT's effectiveness, noting that appropriately challenging task practice drives neuroplastic changes in motor cortex and associated networks[46].
Durairaj et al., (2025) conducted a scoping review of motor learning principles reported in stroke trials of upper limb task-oriented training. The review identified optimal challenge as a key motor learning principle, noting that many successful task-oriented training protocols incorporated systematic difficulty progression and individualized task selection to maintain appropriate challenge. However, the review also noted that many studies failed to explicitly describe how challenge was calibrated or adjusted, highlighting a gap in the reporting and implementation of optimal challenge principles in task-oriented practice[47].
Pollock et al., (2014) used the Challenge Point Framework to guide motor learning of stepping reactions for improved balance control in stroke survivors, providing detailed case examples of how CPF principles can be applied to task-oriented balance training. The cases demonstrated systematic progression of task difficulty based on patient performance, with therapists adjusting parameters such as step distance, speed requirements, and dual-task demands to maintain optimal challenge[22].
Task-oriented practice typically implements optimal challenge through: (1) careful selection of functional tasks matched to patient goals and abilities, (2) systematic manipulation of task parameters such as object properties, spatial requirements, and temporal constraints, (3) progression through hierarchies of task difficulty as patients improve, (4) incorporation of variable practice conditions to enhance learning, and (5) provision of appropriate feedback and guidance to support success while maintaining challenge. Unlike technology-based interventions, task-oriented practice often relies on therapist judgment and experience to calibrate and adjust difficulty, though recent work has begun to develop more systematic approaches to difficulty matching.
RESULTS
Evidence for Adaptive vs Fixed Difficulty: A central question addressed by the literature is whether adaptive difficulty adjustment produces superior outcomes compared to fixed-difficulty training. Multiple studies provide evidence supporting the superiority of adaptive approaches.
Lotay et al., (2019) demonstrated that stroke patients training with Challenge Point Framework-based adaptive scheduling performed better than those training with fixed conditions, though this effect was not observed in healthy volunteers performing near ceiling[20]. This finding suggests that adaptive difficulty is particularly beneficial for individuals with impairments who are operating below ceiling performance. Woodbury et al., (2016) provided proof-of-concept evidence that matching task difficulty to patient ability during task practice improves upper extremity motor skill after stroke compared to standard practice[45]. The study's systematic approach to difficulty matching demonstrated that individualized calibration of challenge produces measurable benefits in motor outcomes.
Metzger et al., (2014) showed that an adaptive robot-assisted therapy system maintaining performance around a 70% success target was feasible and well-received by stroke patients[32]. While the pilot study did not include a fixed-difficulty control group, the successful maintenance of performance within the target range and positive patient feedback supported the adaptive approach. Zimmerli et al., (2012) validated a mechanism to balance exercise difficulty in robot-assisted rehabilitation, demonstrating that adaptive difficulty successfully maintained performance within target ranges and was associated with motor improvements[33].
Olsen et al., (2023) systematic review and meta-analysis of treadmill interventions provided population-level evidence that higher challenge levels are associated with greater improvements in gait outcomes[43]. The meta-analysis found that interventions incorporating higher challenge through faster speeds, incline, or reduced support produced larger effect sizes for gait speed and walking capacity compared to lower-challenge interventions. This dose-response relationship between challenge level and outcomes supports the importance of maintaining appropriate challenge in gait training.
Several studies compared adaptive robotic assistance to fixed assistance levels. Squeri et al., (2012) demonstrated that concurrent regulation of task difficulty and degree of assistance allowed severely impaired stroke survivors to engage in meaningful practice that would not be possible with fixed difficulty or assistance levels[48]. Wang et al., (2022) showed that adaptive control of both task difficulty and robotic assistance promoted motor learning more effectively than fixed parameters[35]. These findings suggest that adaptive approaches are particularly important for patients with severe impairments who require substantial assistance initially but can benefit from progressive challenge increases as they improve.
The comparative evidence consistently supports adaptive difficulty adjustment over fixed approaches, with benefits observed across multiple intervention modalities including robot-assisted therapy, task-oriented practice, and treadmill training. The magnitude of benefit appears to be greatest for patients with moderate to severe impairments, where the gap between current ability and task demands is substantial and requires careful calibration.
Optimal Success Rate Targets: A practical question for implementing optimal challenge is determining the target success rate that defines the Goldilocks Zone. Several studies in this review investigated specific success rate targets.
Metzger et al., (2014) implemented a 70% success rate target in their adaptive hand rehabilitation robot, based on motor learning literature suggesting this represents an optimal balance between challenge and achievable success[32]. The system successfully maintained patient performance around this target, and patients reported appropriate challenge levels. This 70% target has theoretical grounding in the Challenge Point Framework, which suggests that moderate success rates (neither too high nor too low) optimize the interpretive processing required for learning.
Brown et al., (2016) discussed the principle of designing robots that challenge to optimize motor learning, emphasizing that success rates in the 60-80% range appear to maximize learning across various motor tasks[49]. This range provides sufficient success to maintain motivation and activate reward circuits while ensuring enough challenge to drive skill refinement and neuroplastic changes. Success rates above 80-90% may indicate insufficient challenge, while rates below 50-60% may indicate excessive difficulty leading to frustration and maladaptive strategies.
Several studies implemented adaptive algorithms targeting performance within specific ranges rather than fixed success rates. Zimmerli et al., (2012) adjusted difficulty to maintain performance within a target range, allowing for some variability while preventing performance from drifting too far from the optimal zone[33]. This approach recognizes that optimal challenge may vary somewhat across individuals and contexts, and that maintaining performance within a range rather than at a fixed point may be more practical and effective.
The success rate target literature suggests that the optimal zone is relatively broad (approximately 60-80% success) rather than a precise point, and that maintaining performance within this range is more important than hitting a specific target. The optimal target may also vary depending on the specific task, patient characteristics, and rehabilitation goals. For example, tasks emphasizing accuracy may benefit from slightly higher success rates (70-80%) to reinforce correct movement patterns, while tasks emphasizing problem-solving or adaptability may benefit from slightly lower success rates (60-70%) to promote exploration and cognitive engagement.
Mechanisms of Difficulty Adaptation: The literature reveals diverse mechanisms for implementing difficulty adaptation across different intervention modalities. Understanding these mechanisms is critical for translating optimal challenge principles into clinical practice.
In robot-assisted therapy, difficulty adaptation typically involves modulating multiple parameters including: (1) the degree of robotic assistance or resistance provided, (2) the size and location of movement targets, (3) the speed requirements for task completion, (4) the accuracy tolerances for successful performance, and (5) the complexity of movement trajectories. Metzger et al., (2014) adjusted exercise parameters including range of motion requirements, force thresholds, and timing constraints based on patient performance[32]. Squeri et al., (2012) implemented concurrent regulation of task difficulty and assistance level, increasing task demands while reducing assistance as patients improved[48]. Wang et al., (2022) developed a comprehensive control framework that optimized the balance between task difficulty and robotic support based on a computational model of motor learning[35].
In virtual reality and gaming interventions, difficulty adaptation mechanisms include: (1) adjusting target size, speed, or trajectory, (2) modulating the number and behavior of obstacles or distractors, (3) varying time limits for task completion, (4) scaling cognitive demands through dual-task requirements, and (5) adjusting feedback specificity and frequency. Grimm et al., (2016) implemented closed-loop adaptation that adjusted multiple task parameters in real-time based on performance metrics[34]. Lobo (2024) developed a systematic framework for dynamic difficulty adjustment in serious games that considered multiple dimensions of challenge[41].
In treadmill and gait training, difficulty adaptation mechanisms include: (1) progressive increases in walking speed, (2) gradual reduction of body weight support, (3) introduction of incline or decline, (4) addition of dual-task cognitive or motor challenges, and (5) incorporation of perturbations or obstacles. Olsen et al., (2023) meta-analysis identified these challenge-increasing mechanisms and demonstrated their association with improved outcomes[43]. Forrester et al., (2011) adjusted the difficulty of ankle movement tasks during robotic gait training based on patient performance[44].
In task-oriented practice, difficulty adaptation mechanisms include: (1) manipulation of object properties (size, weight, shape), (2) adjustment of spatial requirements (reach distance, target location), (3) modification of temporal constraints (speed requirements, time limits), (4) variation of environmental context (support surface, lighting, distractions), and (5) progression through task hierarchies. Woodbury et al., (2016) systematically adjusted these parameters to match task difficulty to patient ability[45]. Platz et al., (2018) described the systematic difficulty progression in Arm Ability Training[46].
Common across these diverse mechanisms is the principle of multi-dimensional difficulty adjustment. Effective adaptive systems typically modulate multiple task parameters simultaneously to maintain optimal challenge, recognizing that difficulty is not a single dimension but emerges from the interaction of multiple task and environmental factors. Additionally, most successful systems implement gradual, incremental difficulty adjustments rather than large discrete changes, allowing patients to adapt progressively to increasing demands.
Outcomes across Impairment Levels: An important consideration is whether optimal challenge principles apply equally across the spectrum of stroke severity, from mild to severe impairments. The literature provides evidence that adaptive difficulty is beneficial across impairment levels, though the specific implementation may differ.
For severely impaired patients, several studies demonstrated that adaptive systems enabling meaningful practice that would otherwise be impossible are particularly valuable. Squeri et al., (2012) developed a system specifically for severely impaired stroke survivors that provided substantial robotic assistance initially while maintaining appropriate challenge through task difficulty modulation[48]. The system allowed severely impaired patients to engage in active practice by providing the support necessary for task completion while ensuring tasks remained challenging. Choi et al., (2009) developed an adaptive automated robotic system that accommodated a wide range of impairment levels through flexible adjustment of both assistance and task difficulty[50].
For moderately impaired patients, the literature suggests that adaptive difficulty is critical for maintaining engagement and promoting continued improvement. Metzger et al., (2014) studied in subacute stroke patients with moderate impairments demonstrated that adaptive difficulty maintained appropriate challenge throughout recovery[32]. Woodbury et al., (2016) studied in patients with moderate upper extremity impairments showed that difficulty matching improved motor skill acquisition[45]. These studies suggest that the middle range of impairment where patients have some functional capacity but substantial room for improvement may be where optimal challenge principles have the greatest impact.
For mildly impaired patients, the literature provides less direct evidence, though several studies suggest that maintaining challenge remains important to prevent plateaus and promote continued refinement of motor skills. Lotay et al., (2019) found that adaptive difficulty based on Challenge Point Framework principles benefited stroke patients but not healthy volunteers performing near ceiling, suggesting that once patients approach normal function, the benefits of adaptive difficulty may diminish. However, this does not imply that challenge is unimportant for mildly impaired patients, but rather that the challenge must come from increasingly complex, functional tasks rather than basic movement parameters[20].
The literature also suggests that optimal challenge principles may be particularly important during specific phases of recovery. Several studies focused on subacute stroke patients (within the first 6 months post-stroke), a period characterized by rapid spontaneous recovery and heightened neuroplasticity. Maintaining optimal challenge during this critical window may maximize the benefits of rehabilitation. However, studies in chronic stroke patients (>6 months post-stroke) also demonstrated benefits of adaptive difficulty, suggesting that optimal challenge principles remain relevant throughout the recovery trajectory [Table. 1].
| Author (Year) | Intervention Type | Population | Key Findings | Success Rate / Challenge Target | Outcome Measures |
|---|---|---|---|---|---|
| Lotay, et al. (2019) | CPF-based adaptive self-exercise scheduling | Stroke patients & healthy volunteers | Adaptive scheduling benefited stroke patients but not healthy volunteers near ceiling performance | Not specified | Motor performance scores |
| Woodburry, et al. (2016) | Task-oriented upper extremity practice | Stroke patients with UE impairment | Matching task difficulty to patient ability improved upper extremity motor skill vs standard practice | Not specified | Upper extremity motor skill |
| Metzger, et al. (2014) | Robot-assisted hand rehabilitation | Subacute stroke patients | Adaptive system maintaining 70% success target was feasible, well-received and maintained performance within target range | 70% | Feasibility, patient-reported challenge, motor performance |
| Zimmerli, et al. (2012) | Robot-assisted upper extremity rehabilitation | Stroke patients | Validated adaptive mechanism successfully maintained performance within target ranges; associated with motor improvements | Target range maintained | Motor improvement, exercise balance validation |
| Olsen, et al. (2023) | Treadmill training (SR & MA) | Stroke patients | Higher challenge levels (faster speeds, incline, reduced support) associated with greater gait improvement; dose-response relationship confirmed | Higher challenge larger = larger effect size | Gait speed, walking capacity |
| Squeri, et al. (2012) | Robot-assisted therapy (BioRob) | Severely impaired stroke survivors | Concurrent regulation of task difficulty and assistance level enabled meaningful practice impossible with fixed parameters | Not specified | Engagement in active practice, motor performance |
| Brown, et al. (2016) | Robotic therapy design principles | Theoretical/ design framework | Success rates of 60-80% maximize motor learning; above 80-90% insufficient challenge; below 50-60% excessive difficulty | 60-80% | Motor learning (theoretical) |
| Wang, et al. (2022) | Upper limb rehabilitation robot (adaptive control) | Stroke patients | Adaptive control framework optimizing task difficulty and robotic assistance promoted motor learning more effectively than fixed parameters | Not specified | Motor learning outcomes, control framework validation |
| Grimm, et al. (2016) | VR reach to grasp with exoskeleton | Stroke patients | Closed-loop adaptation of task difficulty in real-time based on performance metrices improved rehabilitation outcomes | Not specified | Reach to grasp performance, neurophysiological measures |
| Lobo P H (2024) | Dynamic difficulty adjustment in serious games | Neurorehabilitation population | Systematic multi-dimensional framework for dynamic difficulty adjustment developed for serious games in neurorehabilitation | Not specified | Framework validation, game performance metrices |
| Platz, et al. (2018) | Arm ability training (AAT) | Stroke patients with dexterity impairment | Systematic difficulty progression in AAT promotes dexterity recovery; reviewed clinical effectiveness and neurobiological mechanisms | Systematic progression | Dexterity outcomes, neurobiological evidence |
| Choi, et al. (2009) | Adaptive automated robotic task-practice | Stroke patients across impairment levels | Adaptive robotic system accommodated wide range of impairment levels through flexible adjustment of assistance and task difficulty | Not specified | Arm function, adaptability across impairment severity |
Table 1: Summary table of the key findings
| First Author (Year) |
Clarity of Objectives (0–2) |
Methodological Rigour (0–2) |
Sample Size Adequacy (0–2) |
Outcome Measure Validity (0–2) |
Statistical Analysis (0–2) |
Generalisability (0–2) |
Clinical Relevance (0–2) |
Limitations Discussed (0–2) |
Replicability (0–2) |
Evidence Level (0–2) |
Total Score (20) |
Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lotay, et al. (2019) | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 13 | Moderate |
| Woodbury et al. (2016) | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 15 | High |
| Metzger et al. (2014) | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 14 | Moderate |
| Zimmerli et al. (2012) | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 15 | High |
| Olsen et al. (2023) | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 | High |
| Squeri et al. (2012) | 1 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 0 | 2 | 10 | Moderate |
| Brown et al. (2016) | 2 | 1 | 0 | 1 | 0 | 2 | 2 | 1 | 1 | 2 | 12 | Moderate |
| Wang et al. (2022) | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 | High |
| Grimm et al. (2016) | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 16 | High |
| Lobo PH (2024) | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 11 | Moderate |
| Platz & Lotze (2018) | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 16 | High |
| Choi, et al. (2009) | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 18 | High |
| Each Criteria rated as: 0-absent/poor, 1-partial, 2- fully met | Quality: ≥ 15 High, 10-14 Moderate, <10 Low | |||||||||||
Table 2: Article quality assessment summary
DISCUSSION
Synthesis of Evidence: Taken together, the available evidence suggests several convergent themes, though the largely preliminary nature of the included studies necessitates that these be treated as indicative rather than definitive findings.
First, available evidence suggests that adaptive difficulty adjustment may support superior motor learning outcomes compared to fixed-difficulty approaches across multiple intervention modalities, including robot-assisted therapy, virtual reality, treadmill training and task-oriented practice. Studies directly comparing adaptive to fixed difficulty reported benefits in motor function, skill acquisition and engagement, though many were underpowered and lacked robust controls[20, 45]. Meta-analytic evidence from treadmill training showed a dose-response relationship between challenge level and gait outcomes[43]. This convergent pattern across diverse methodologies and outcome measures suggests that maintaining optimal challenge is an important principle in stroke rehabilitation, though the preliminary and heterogenous
nature of many included studies warrants cautious interpretation pending larger confirmatory trials.
Second, the optimal challenge zone appears to correspond to success rates in the 60-80% range, with 70% emerging as a common target in the literature[32, 49]. This range represents a balance between sufficient challenge to drive learning and neuroplasticity, and sufficient success to maintain motivation and reinforce correct movement patterns. The relatively broad optimal range (rather than a precise point) suggests that maintaining performance within this zone is more important than hitting a specific target, and that some individual variability in optimal challenge is expected and acceptable.
Third, effective implementation of optimal challenge requires multi-dimensional difficulty adjustment, continuous performance monitoring, and individualized calibration. Successful adaptive systems modulate multiple task parameters simultaneously (e.g., speed, accuracy requirements, assistance level, complexity) rather than adjusting a single dimension[35, 48]. Real-time performance assessment enables responsive difficulty adjustment that maintains patients within their optimal zone as skills develop[34]. Initial difficulty calibration based on comprehensive assessment ensures appropriate starting points for individual patients[32].
Fourth, optimal challenge principles appear to be beneficial across the spectrum of stroke severity, though implementation differs based on impairment level. For severely impaired patients, adaptive systems that provide substantial assistance while maintaining task challenge enable meaningful practice that would otherwise be impossible[48, 50]. For moderately impaired patients, adaptive difficulty maintains engagement and promotes continued improvement through the recovery process[32, 45]. The evidence suggests that the middle range of impairment may be where optimal challenge principles have the greatest impact, though benefits extend across the severity spectrum.
Fifth, the theoretical foundation for optimal challenge is well-established in motor learning science, particularly the Challenge Point Framework, which provides a principled basis for understanding how task difficulty and learner skill interact to determine learning outcomes[1, 2]. The neurobiological basis lies in activity-dependent neuroplasticity, with appropriately challenging practice driving neural reorganization and functional recovery[27, 29]. The convergence of theoretical, neurobiological, and preliminary empirical evidence provides a promising foundation for the Goldilocks Zone concept in neurorehabilitation, though definitive conclusions await adequately power trials.
Theoretical Basis and Implications:The evidence reviewed has several important theoretical implications for understanding motor learning and recovery after stroke. The consistent benefits of adaptive difficulty across diverse interventions suggest that optimal challenge is a fundamental principle of motor learning rather than a modality-specific phenomenon. Whether implemented through robotic assistance, virtual reality, treadmill training, or task-oriented practice, maintaining appropriate challenge appears to be a critical determinant of learning outcomes. This universality suggests that optimal challenge should be considered a core principle in rehabilitation theory and practice[35, 36].
The success of adaptive approaches challenges traditional rehabilitation paradigms that often employ standardized protocols with fixed difficulty progressions. The evidence suggests that individualized, responsive difficulty adjustment based on continuous performance monitoring is superior to predetermined progression schedules. This has implications for how rehabilitation protocols are designed and implemented, emphasizing the need for flexibility and personalization rather than rigid standardization[32, 33].
The integration of Challenge Point Framework principles with neuroplasticity research provides a comprehensive theoretical model linking behavioral practice parameters to neural mechanisms of recovery. The CPF explains how task difficulty and learner skill interact to determine the cognitive processing required for learning, while neuroplasticity research explains how this processing drives neural reorganization. This integrated model provides a mechanistic understanding of why optimal challenge is critical for recovery and offers guidance for optimizing rehabilitation interventions[37, 39].
The concept of virtuous and vicious cycles in arm use and function extends optimal challenge principles beyond individual practice sessions to consider the broader context of daily living and long-term recovery. This perspective suggests that rehabilitation must not only provide optimal challenge during therapy sessions but also promote sufficient arm use in daily activities to maintain a virtuous cycle of use and function. This has implications for home-based rehabilitation, self-practice, and the transition from formal therapy to independent function[27, 29].
The motivational dimensions of optimal challenge including the promotion of engagement, promoting flow states, and reward-circuit activation underscore the importance of attending to psychological as well as biomechanical factors in rehabilitation design. The Goldilocks Zone concept thus extends beyond motor learning theory to encompass motivational science, reinforcing the view that effective rehabilitation must address both the physical and psychological determinants of recovery.
Methodological Considerations and Limitations of the Evidence: Several methodological considerations are important for interpreting the evidence base of this review. A key limitation is that the majority of included studies were pilot studies, feasibility investigations, or non-randomised designs with small samples, substantially limiting statistical power, generalisability and the ability to draw causal inferences. These studies offer valuable proof-of-concept data and demonstrate feasibility but are insufficient to establish efficacy. Findings should therefore be interpreted as preliminary and hypothesis-generating rather than conclusive. Larger, adequately powered randomised controlled trials with active control conditions are required before definitive clinical recommendations can be made.
There is substantial heterogeneity in how optimal challenge is operationalized and measured across studies. Some studies target specific success rates, others adjust difficulty based on performance thresholds, and still others use therapist judgment to calibrate challenge[32, 33, 45]. This heterogeneity makes it difficult to compare findings across studies and synthesize evidence about optimal implementation approaches. Greater standardization in how optimal challenge is defined, measured, and implemented would facilitate evidence synthesis and clinical translation.
Outcome measures vary widely across studies, including impairment-level measures (e.g., Fugl-Meyer Assessment), activity-level measures (e.g., Action Research Arm Test, gait speed), and participation-level measures (e.g., quality of life, community integration). While this diversity reflects the multidimensional nature of stroke recovery, it complicates efforts to determine which outcomes are most sensitive to optimal challenge interventions and which are most clinically meaningful. Future research should include comprehensive outcome batteries spanning multiple levels of the International Classification of Functioning, Disability and Health (ICF) framework.
Studies focus on short-term outcomes measured immediately post-intervention or at short follow-up periods. Fewer studies examine long-term retention of gains or the durability of benefits from optimal challenge interventions. Given that stroke rehabilitation aims to produce lasting functional improvements, longer-term follow-up studies are critical for establishing the sustained benefits of adaptive difficulty approaches.
Most studies examine optimal challenge in the context of supervised, clinic-based rehabilitation. Fewer studies have investigated how optimal challenge principles can be implemented in home-based or self-directed rehabilitation, despite the importance of continued practice outside formal therapy sessions. Research on technology-enabled home rehabilitation with adaptive difficulty is an important direction for extending optimal challenge principles beyond the clinic.
There is limited evidence comparing different adaptive algorithms or difficulty adjustment strategies. While many studies demonstrate that adaptive difficulty is superior to fixed difficulty, fewer studies compare different approaches to implementing adaptation (e.g., success rate targets vs. performance thresholds, single-parameter vs. multi-parameter adjustment, continuous vs. discrete difficulty changes). Comparative effectiveness research examining different adaptive strategies would inform optimal implementation.
Clinical Implications and Recommendations: The evidence reviewed has important implications for implementing optimal challenge principles in clinical stroke rehabilitation practice. Clinicians should adopt an individualized, assessment-driven approach to difficulty calibration. Initial difficulty should be based on comprehensive assessment of patient capabilities across relevant domains (motor, sensory, cognitive) rather than standardized starting points[32]. This requires developing or adopting assessment tools that provide sufficient detail to inform difficulty calibration and that can be efficiently administered in clinical settings.
Clinicians should implement systematic, continuous monitoring of patient performance to guide difficulty adjustment. Rather than relying solely on periodic formal assessments, clinicians should track performance metrics during each practice session (e.g., success rates, movement quality, effort level) and use these data to adjust difficulty responsively[33]. This requires developing practical methods for performance tracking that do not impose excessive burden on clinicians or interrupt the flow of therapy.
Difficulty adjustment should be multi-dimensional, modulating multiple task parameters to maintain optimal challenge. Clinicians should consider adjusting object properties, spatial requirements, temporal constraints, environmental context, and the degree of assistance or guidance provided[45, 46]. This multi-dimensional approach allows for fine-grained calibration of challenge and prevents patients from reaching ceiling on any single dimension while other dimensions remain unchallenged.
Clinicians should target success rates in the 60-80% range as a practical heuristic for optimal challenge, adjusting difficulty when performance consistently falls outside this range[32, 49]. While individual patients may have somewhat different optimal zones, this range provides a reasonable starting point. Clinicians should also attend to qualitative indicators of appropriate challenge including patient engagement, effort level, and emotional responses (frustration vs. satisfaction).
Difficulty progression should be gradual and incremental rather than large discrete jumps. Small, frequent difficulty increases allow patients to adapt progressively to increasing demands and reduce the risk of overwhelming patients with excessive challenge[33]. This principle of gradual progression applies across all intervention modalities and should be a standard feature of rehabilitation protocols.
Clinicians should explicitly discuss optimal challenge principles with patients, explaining the rationale for difficulty adjustments and involving patients in the process of calibrating challenge. Patient input on perceived difficulty, effort, and satisfaction can complement objective performance metrics in guiding difficulty adjustment. This collaborative approach promotes patient engagement and self-efficacy.
Technology plays a critical role in enabling systematic implementation of optimal challenge principles, offering capabilities for objective performance measurement, automated difficulty adjustment, and data-driven decision support. Several recommendations emerge for technology integration in clinical practice.
Rehabilitation technologies should incorporate adaptive difficulty algorithms as a core feature rather than an optional add-on. The evidence clearly supports adaptive over fixed difficulty, suggesting that adaptive capability should be a standard requirement for rehabilitation technologies[20, 33, 34]. Technology developers should prioritize implementing robust, validated adaptive algorithms in robotic systems, virtual reality platforms, and other rehabilitation technologies.
Technologies should provide clinicians with clear, actionable performance data to inform difficulty adjustment decisions. User interfaces should display key metrics such as success rates, movement quality indicators, and performance trends in formats that are easily interpretable and support clinical decision-making[32]. Data visualization tools that show performance relative to target ranges or optimal zones can help clinicians quickly assess whether difficulty adjustments are needed. Technologies should allow for flexible, clinician-controlled difficulty adjustment in addition to automated adaptation. While automated algorithms can handle routine difficulty adjustments, clinicians should retain the ability to override automated decisions based on clinical judgment, patient feedback, or other contextual factors[33]. This hybrid approach combines the efficiency of automation with the expertise and contextual awareness of clinicians.
Technologies should support home-based rehabilitation with adaptive difficulty, extending optimal challenge principles beyond clinic-based therapy. Home rehabilitation systems should incorporate simplified adaptive algorithms that can function with minimal supervision while providing data to clinicians for remote monitoring and adjustment[49]. This extends the dose of appropriately challenging practice beyond formal therapy sessions. Technologies should be designed with implementation barriers in mind, including cost, setup time, training requirements, and integration with clinical workflows. Even highly effective technologies will have limited impact if implementation barriers prevent widespread adoption. Technology developers should engage with clinicians and healthcare systems throughout the development process to ensure technologies are practical and feasible for real-world clinical use.
Effective implementation of optimal challenge requires robust personalization based on comprehensive assessment of individual patient characteristics. Several recommendations address personalization and assessment. Rehabilitation programs should incorporate comprehensive baseline assessments that evaluate motor, sensory, cognitive, and psychological factors relevant to task performance and learning. These assessments should provide sufficient detail to inform initial difficulty calibration across multiple task dimensions[32]. Standardized assessment batteries that are efficient to administer and provide actionable data for difficulty calibration would facilitate implementation.
Assessment should be ongoing throughout rehabilitation, not limited to baseline and outcome time points. Frequent assessment enables responsive difficulty adjustment and allows for detection of plateaus or declines that may require intervention modifications[33]. Technologies that embed assessment within practice activities (e.g., robotic systems that measure performance during therapy) can reduce assessment burden while providing continuous data.
Personalization should consider not only current performance levels but also individual learning rates, recovery trajectories, and response to different types of challenge. Some patients may benefit from more aggressive difficulty progression, while others may require more gradual increases[38]. Adaptive algorithms that learn individual patient characteristics and adjust difficulty accordingly represent an important direction for personalized rehabilitation. It should extend beyond impairment-level factors to consider patient goals, preferences, and life contexts. Optimal challenge in task-oriented practice should be calibrated relative to tasks that are meaningful and relevant to individual patients' daily activities and participation goals[45, 46]. This patient-centered approach ensures that rehabilitation addresses outcomes that matter to patients.
Assessment and personalization should consider the multidimensional nature of stroke recovery, including motor, cognitive, emotional, and social factors. Optimal challenge in one domain (e.g., motor difficulty) may need to be balanced against challenges in other domains (e.g., cognitive load, emotional stress). Comprehensive assessment and personalization should consider these interactions and optimize challenge across multiple dimensions simultaneously.
Future Directions: Several important directions for future research emerge from this scoping review. Large-scale randomized controlled trials are needed to definitively establish the efficacy of adaptive difficulty approaches compared to standard care and to determine optimal implementation parameters. While pilot studies and feasibility studies provide important preliminary evidence, adequately powered trials with rigorous methodology are necessary to establish evidence-based recommendations for clinical practice. Research is needed to compare different adaptive algorithms and difficulty adjustment strategies. Questions include: What is the optimal target success rate or performance range? How frequently should difficulty be adjusted? Should adjustment be continuous or discrete? Should multiple task parameters be adjusted simultaneously or sequentially? How should adaptive algorithms balance different dimensions of challenge? Comparative effectiveness research addressing these questions would inform optimal implementation.
Research should investigate how optimal challenge principles can be effectively implemented in home-based and community-based rehabilitation settings. Most current evidence comes from supervised, clinic-based interventions, but extending optimal challenge to home practice could substantially increase rehabilitation dose and improve outcomes. This requires developing technologies and protocols that enable adaptive difficulty with minimal supervision while ensuring safety and effectiveness. Research should examine the long-term effects of optimal challenge interventions, including retention of gains, durability of benefits, and impact on long-term functional outcomes and quality of life. Most current studies examine short-term outcomes, but stroke rehabilitation aims to produce lasting improvements. Longer follow-up periods (6-12 months or more) are needed to establish sustained benefits.
Research should investigate individual differences in optimal challenge, including how factors such as age, stroke severity, cognitive status, motivation, and psychological factors influence the optimal difficulty level and progression rate. Understanding these individual differences would enable more sophisticated personalization of difficulty adjustment and identification of patients most likely to benefit from adaptive approaches. Research should examine the mechanisms underlying the benefits of optimal challenge, including neuroimaging studies investigating how appropriately challenging practice drives neural reorganization and behavioral studies examining the cognitive and motivational processes engaged by optimal challenge. Mechanistic research would deepen theoretical understanding and potentially identify biomarkers or predictors of response to optimal challenge interventions.
Research should investigate how optimal challenge principles can be integrated with other evidence-based rehabilitation approaches such as constraint-induced movement therapy, intensive task-specific training, and aerobic exercise. Understanding how optimal challenge interacts with other therapeutic principles would enable development of comprehensive, multi-component interventions that maximize recovery. Research should examine the cost-effectiveness of adaptive difficulty interventions, including the costs of technologies, training, and implementation balanced against the benefits in terms of improved outcomes, reduced disability, and enhanced quality of life. Cost-effectiveness evidence is critical for healthcare decision-making and resource allocation.
Research should investigate implementation science questions related to adopting optimal challenge principles in clinical practice, including barriers and facilitators to implementation, effective training and education strategies for clinicians, and organizational factors that support or hinder adoption. Understanding implementation challenges is critical for translating research evidence into widespread clinical practice. Research should explore the application of artificial intelligence and machine learning approaches to optimize difficulty adjustment. Machine learning algorithms could potentially learn optimal difficulty adjustment strategies from large datasets of patient performance, identifying patterns and predictive factors that inform more sophisticated personalization. This represents an exciting frontier for advancing adaptive rehabilitation technologies.
CONCLUSION
This scoping review mapped evidence suggesting that optimal challenge, the Goldilocks Zone is a theoretically well-grounded and clinically promising concepts in stroke neurorehabilitation. Drawing on the challenge point framework and activity-dependent neuroplasticity, adaptively calibrated task difficulty appears to support motor learning and functional recovery across multiple intervention modalities. Preliminary evidence indicates that targeting success rate in the 60-80% range with individualised, multi-dimensional difficulty adjustment is both feasible and potentially beneficial. However, the majority of included studies were pilot or feasibility investigations with small samples and limited methodological controls; accordingly, definitive efficacy conclusions are premature. Well-powered randomised controlled trials with standardised outcome batteries and longer follow-up periods are needed before firm clinical recommendations can be advanced. The theoretical coherence of the Goldilocks Zone concepts and the consistency of early findings across diverse modalities provide a meaningful foundation for future investigation and cautious clinical application, with the ultimate goal of advancing personalised, adaptive neurorehabilitation for stroke survivors.
DISCLOSURE
Funding: Nil.
Conflict of Interest: None.
References
References
1. Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J, Lindsay P, <I>et al</I>. World Stroke Organization: Global Stroke Fact Sheet 2025. International Journal of Stroke. 2025; 20 (2). Available from: https://doi.org/10.1177/17474930241308142
2. GBD 2019 Stroke Collaborators. Global, regional and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study. Lancet Neurology. 2021; 20 (10). Available from: https://doi.org/https://doi.org/10.1016/s1474-4422(21)00252-0
3. Cramer SC, Sur M, Dobkin BH, O’Brien C, Sanger TD, Trojanowski JQ, <I>et al</I>. Harnessing neuroplasticity for clinical applications. Brain. 2011; 134 (6). Available from: https://doi.org/10.1093/brain/awr039
4. Kleim JA, Jones TA. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation After Brain Damage. Journal of Speech, Language, and Hearing Research. 2008; 51 (1). Available from: https://doi.org/10.1044/1092-4388(2008/018)
5. Guadagnoli MA, Lee TD. Challenge Point: A Framework for Conceptualizing the Effects of Various Practice Conditions in Motor Learning. Journal of Motor Behavior. 2004; 36 (2). Available from: https://doi.org/10.3200/jmbr.36.2.212-224
6. Reiss AP, Wolf SL, Hammel EA, McLeod EL, Williams EA. Constraint-Induced Movement Therapy (CIMT): Current Perspectives and Future Directions. Stroke Research and Treatment. 2012; 2012 Available from: https://doi.org/10.1155/2012/159391
7. Wolf SL, Thompson PA, Winstein CJ, Miller JP, Blanton SR, Nichols- Larsen DS, <I>et al</I>. The EXCITE stroke trial: comparing early and delayed constraint-induced movement therapy. Stroke. 2010; 41 (10). Available from: https://doi.org/10.1161/strokeaha.110.588723
8. Levin MF, Kleim JA, Wolf SL. What Do Motor “Recovery” and “Compensation” Mean in Patients Following Stroke?. Neurorehabilitation and Neural Repair. 2009; 23 (4). Available from: https://doi.org/10.1177/1545968308328727
9. Onla-or S, Winstein CJ. Determining the Optimal Challenge Point for Motor Skill Learning in Adults With Moderately Severe Parkinson's Disease. Neurorehabilitation and Neural Repair. 2008; 22 (4). Available from: https://doi.org/10.1177/1545968307313508
10. Kitago T, Krakauer JW. Motor learning principles for neurorehabilitation. Handbook of Clinical Neurology. 2013; 110 Available from: https://doi.org/10.1016/b978-0-444-52901-5.00008-3
11. Kleynen B, Braun SM, Bleijlevens MH, Lexis MA, Rasquin SM, Halfens J, <I>et al</I>. Using a Delphi Technique to Seek Consensus Regarding Definitions, Descriptions and Classification of Terms Related to Implicit and Explicit Forms of Motor Learning. PLoS ONE. 2014; 9 (6). Available from: https://doi.org/10.1371/journal.pone.0100227
12. Mehrholz J, Pohl M, Platz T, Kugler J, Elsner B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database of Systematic Reviews. 2018; 2018 (9). Available from: https://doi.org/10.1002/14651858.cd006876.pub5
13. Maggio MG, Latella D, Maresca G, Sciarrone F, Manuli A, Naro A, <I>et al</I>. Virtual Reality and Cognitive Rehabilitation in People With Stroke: An Overview. Journal of Neuroscience Nursing. 2019; 51 (2). Available from: https://doi.org/10.1097/jnn.0000000000000423
14. Nann M, Peekhaus N, Angerhofer C, Soekadar SR. Feasibility and Safety of Bilateral Hybrid EEG/EOG Brain/Neural–Machine Interaction. Frontiers in Human Neuroscience. 2020; 14 Available from: https://doi.org/10.3389/fnhum.2020.580105
15. Krakauer JW, Carmichael ST, Corbett D, Wittenberg GF. Getting neurorehabilitation right: what can be learned from animal model?. Neurorehabilitation and Neural Repair. 2012; 26 (8). Available from: https://doi.org/10.1177/1545968312440745
16. Schmidt RA, Wrisberg CA. Motor Learning and Performance: a situation-based learning approach. <I>Human Kinetics</I>. 4th Edition. 2008.
17. Nudo RJ. Recovery after brain injury: mechanisms and principles. Frontiers in Human Neuroscience. 2013; 7 Available from: https://doi.org/10.3389/fnhum.2013.00887
18. Wulf G, Lewthwaite R. Optimizing performance through intrinsic motivation and attention for learning: The OPTIMAL theory of motor learning. Psychonomic Bulletin & Review. 2016; 23 (5). Available from: https://doi.org/10.3758/s13423-015-0999-9
19. Dobkin BH. Training and exercise to drive poststroke recovery. Nature Clinical Practice Neurology. 2008; 4 (2). Available from: https://doi.org/10.1038/ncpneuro0709
20. Lotay R, Mace M, Rinne P, Burdet E, Bently P. optimizing self-exercise scheduling in motor stroke using Challenge Point Framework theory. 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR). 2019; Available from: https://doi.org/10.1109/icorr.2019.8779497
21. Maier M, Ballester BR, Verschure PFMJ. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Frontiers in Systems Neuroscience. 2019; 13 Available from: https://doi.org/10.3389/fnsys.2019.00074
22. Pollock CL, Boyd LA, Hunt MA, Garland SJ. Use of the Challenge Point Framework to Guide Motor Learning of Stepping Reactions for Improved Balance Control in People With Stroke: A Case Series. Physical Therapy. 2014; 94 (4). Available from: https://doi.org/10.2522/ptj.20130046
23. Porter JM, Magill RA. Systematically increasing contextual interference is beneficial for learning sport skills. Journal of Sports Sciences. 2010; 28 (12). Available from: https://doi.org/10.1080/02640414.2010.502946
24. Czyz SH, Wojcik AM, Solarska P, Kiper P. High contextual interference improves retention in motor learning: systematic review and meta-analysis. Scientific Reports. 2024; 14 (1). Available from: https://doi.org/10.1038/s41598-024-65753-3
25. Carmichael ST. Cellular and molecular mechanisms of neural repair after stroke: Making waves. Annals of Neurology. 2006; 59 (5). Available from: https://doi.org/10.1002/ana.20845
26. Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E, Weiller C. Treatment-Induced Cortical Reorganization After Stroke in Humans. Stroke. 2000; 31 (6). Available from: https://doi.org/10.1161/01.str.31.6.1210
27. Smith MC, Stinear CM. Plasticity and motor recovery after stroke: Implications for physiotherapy. New Zealand Journal of Physiotherapy. 2016; 44 (3). Available from: https://doi.org/10.15619/nzjp/44.3.06
28. Wolpert DM, Diedrichsen J, Flanagan JR. Principles of sensorimotor learning. Nature Reviews Neuroscience. 2011; 12 (12). Available from: https://doi.org/10.1038/nrn3112
29. Ballester BR, Winstein C, Schweighofer N. Virtuous and Vicious Cycles of Arm Use and Function Post-stroke. Frontiers in Neurology. 2022; 13 Available from: https://doi.org/10.3389/fneur.2022.804211
30. Taub E, Uswatte G, Mark VW, Morris DM. The learned nonuse phenomenon: implications for rehabilitation. <I>Europa Medicophysica</I>. 2006; 42(3):241-56.
31. Wadden KP, Asis K, Mang CS, Neva JL, Peter S, Lakhani B, <I>et al</I>. Predicting Motor Sequence Learning in Individuals With Chronic Stroke. Neurorehabilitation and Neural Repair. 2017; 31 (1). Available from: https://doi.org/10.1177/1545968316662526
32. Metzger JC, Lambercy O, Califfi A, Dinacci D, Petrillo C, Rossi P, <I>et al</I>. Assessment-driven selection and adaptation of exercise difficulty in robot-assisted therapy: a pilot study with a hand rehabilitation robot. Journal of NeuroEngineering and Rehabilitation. 2014; 11 (1). Available from: https://doi.org/10.1186/1743-0003-11-154
33. Zimmerli L, Krewer C, Gassert R, Müller F, Riener R, Lünenburger L. Validation of a mechanism to balance exercise difficulty in robot-assisted upper-extremity rehabilitation after stroke. Journal of NeuroEngineering and Rehabilitation. 2012; 9 (1). Available from: https://doi.org/10.1186/1743-0003-9-6
34. Grimm F, Naros G, Gharabaghi A. Closed-Loop Task Difficulty Adaptation during Virtual Reality Reach-to-Grasp Training Assisted with an Exoskeleton for Stroke Rehabilitation. Frontiers in Neuroscience. 2016; 10 Available from: https://doi.org/10.3389/fnins.2016.00518
35. Wang C, Peng L, Hou ZG. A Control Framework for Adaptation of Training Task and Robotic Assistance for Promoting Motor Learning With an Upper Limb Rehabilitation Robot. IEEE Transactions on Systems, Man, and Cybernetics: Systems. 2022; 52 (12). Available from: https://doi.org/10.1109/tsmc.2022.3163916
36. Basteris A, Nijenhuis SM, Buurke JH, Prange GB, Amirabdollahian F. Lag–lead based assessment and adaptation of exercise speed for stroke survivors. Robotics and Autonomous Systems. 2015; 73 Available from: https://doi.org/10.1016/j.robot.2014.08.013
37. Pan L, Song A, Wang S, Duan S. Experimental Study on Upper-Limb Rehabilitation Training of Stroke Patients Based on Adaptive Task Level: A Preliminary Study. BioMed Research International. 2019; 2019 (1). Available from: https://doi.org/10.1155/2019/2742595
38. Giang C, Pirondini E, Kinany N, Pierella C, Panarese A, Coscia M, <I>et al</I>. Motor improvement estimation and task adaptation for personalized robot-aided therapy: a feasibility study. Biomedical Engineering Online. 2020; 19 (1). Available from: https://doi.org/10.1101/728725
39. Rubino C, Lakhani B, Larssen BC, Kraeutner SN, Andrushko JW, Borich MR, <I>et al</I>. Gamified Practice Improves Paretic Arm Motor Behavior in Individuals With Stroke. Neurorehabilitation and Neural Repair. 2024; 38 (11-12). Available from: https://doi.org/10.1177/15459683241286449
40. Fridman D. <I>Designing a Game for Upper Limb Rehabilitation Following a Stroke</I>. (Doctoral dissertation, Open Access Te Herenga Waka-Victoria University of Wellington). 2021
41. Lobo PH. <I>A Dynamic Difficulty Adjustment Framework for Serious Games Applications in Neurorehabilitation</I>. (Master's thesis, Universidade da Madeira (Portugal)). 2024
42. Li Y, Song R. Online Regulation of Task Difficulty based on Neuro- and Motor-feedback to improve engagement in Visual-motor Task. IEEE Transactions on Biomedical Engineering. 2025; Available from: https://doi.org/10.1109/tbme.2025.3615733
43. Olsen S, Alder G, Rashid U, Gomes E, Aislabie M, Chee F. Challenge Level Contributes to the Efficacy of Treadmill Interventions after Stroke: A Systematic Review and Meta-Analysis. Brain Sciences. 2023; 13 (12). Available from: https://doi.org/10.3390/brainsci13121729
44. Forrester LW, Roy A, Krebs HI, Macko RF. Ankle Training With a Robotic Device Improves Hemiparetic Gait After a Stroke. Neurorehabilitation and Neural Repair. 2011; 25 (4). Available from: https://doi.org/10.1177/1545968310388291
45. Woodbury ML, Anderson K, Finetto C, Fortune A, Dellenbach B, Grattan E, <I>et al</I>. Matching Task Difficulty to Patient Ability During Task Practice Improves Upper Extremity Motor Skill After Stroke. Archives of Physical Medicine and Rehabilitation. 2016; 97 (11). Available from: https://doi.org/10.1016/j.apmr.2016.03.022
46. Platz T, Lotze M. Arm Ability Training (AAT) Promotes Dexterity Recovery After a Stroke—a Review of Its Design, Clinical Effectiveness, and the Neurobiology of the Actions. Frontiers in Neurology. 2018; 9 Available from: https://doi.org/10.3389/fneur.2018.01082
47. Durairaj S, Sardesai S, Solomon JM, Levin MF. Motor learning principles reported in stroke trials of upper limb task-oriented training: a scoping review. BMJ Open. 2025; 15 (11). Available from: https://doi.org/10.1136/bmjopen-2024-098599
48. Squeri V, Sterpi I, Basteris A, Casadio M, Pisano F, Colombo R, <I>et al</I>. Robot therapy for severely impaired stroke survivors: Toward a concurrent regulation of task difficulty and degree of assistance. 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob). 2012; Available from: https://doi.org/10.1109/biorob.2012.6290847
49. Brown DA, Lee TD, Reinkensmeyer DJ, Duarte JE. Designing Robots That Challenge to Optimize Motor Learning. Neurorehabilitation Technology. 2016; Available from: https://doi.org/10.1007/978-3-319-28603-7_3
50. Choi Y, Gordon J, Kim D, Schweighofer N. An Adaptive Automated Robotic Task-Practice System for Rehabilitation of Arm Functions After Stroke. IEEE Transactions on Robotics. 2009; 25 (3). Available from: https://doi.org/10.1109/tro.2009.2019787
Copyright
© 2026 Published by Laxmi Memorial Education Trust. This is an open-access article under CC BY 4.0 license. (https://creativecommons.org/licenses/by/4.0/)
Cite this article
P G Krishnendu, K B Riyas Basheer, Ismail Hazim, K R Athul Krishna, Subhashchandra Rai. The Goldilocks Zone in Advanced Neurorehabilitation: A Scoping Review on Optimal Challenge in Stroke Recovery. AJ J Med Sci 2026;3(2):38-49