Volume: 3 Issue: 1
The Effect of Eccentric Loading Exercise in Achilles Tendinitis – A Case Study
Year: 2026, Page: 33-37, Doi: https://doi.org/10.71325/ajjms.v3i1.25.78
Received: Oct. 16, 2025 Accepted: Jan. 20, 2026 Published: May 18, 2026
Abstract
Achilles tendinitis is a common musculoskeletal disorder characterized by inflammation and degeneration of the Achilles tendon, which connects calf muscle to the heel bone. This case study is undertaken to evaluate the effectiveness of eccentric loading exercises in reducing pain, improving tendon strength, and enhancing functional outcomes in patients with Achilles tendinitis. 64-year-old male shopkeeper diagnosed with Achilles tendinitis was assessed for pain pre and post intervention using the Visual Analog Scale (VAS). Eccentric loading exercise was given for the duration of 6 weeks. VAS score decreased from 7/10 (pre – intervention) to 3/10 (post-intervention) following the eccentric loading exercise program. Eccentric loading exercise effectively reduced pain in patient with Achilles tendinitis.
Keywords: Achilles tendinitis, Eccentric loading exercise, Visual Analog scale, Pain test
INTRODUCTION
Achilles tendinitis is a common overuse injury characterized by pain, stiffness and reduced functional ability of the Achilles tendon. It is especially prevalent among athletes, particularly runners, accounting for about 5–9% of cases in elite runners, highlighting its significant impact in sports medicine. The etiology of Achilles tendinitis is multifactorial, with overuse, mechanical overload, and repetitive stress being the primary contributors that cause microtrauma and inflammation. Intrinsic factors such as biomechanical abnormalities, overpronation, and tight calf muscles, along with extrinsic factors like improper footwear and sudden changes in training intensity, can further aggravate the condition[1].
The Achilles tendon is formed by the convergence of the gastrocnemius and soleus muscles. The soleus muscle lies deep to the gastrocnemius and originates from the posterior surface of the upper tibia. The tendon inserts into the posterior surface of the calcaneus, just below the posterior- superior calcaneal tuberosity. Unlike other tendons, the Achilles tendon is not enclosed within a true synovial sheath but is surrounded by a paratenon consisting of a single layer of cells. This paratenon connects to the tendon through a series of transverse vincula that serve as passageways for blood vessels. Additionally, the Achilles tendon receives its blood supply from vessels that arise at the musculotendinous and osteotendinous junctions[2].
Clinically, patients with Achilles tendinitis typically present with pain and stiffness in the posterior aspect of the ankle, which worsens with activity and improves with rest. Morning stiffness and tenderness along the tendon, especially at its insertion on the calcaneus, are characteristic findings. In chronic cases, swelling and crepitus may also be present[1].
The causes and mechanisms of Achilles tendinitis can be classified into intrinsic and extrinsic factors: Intrinsic factors include anatomical abnormalities, age, sex, metabolic dysfunction, foot deformities, limb length discrepancy (dysmetria), muscle weakness or imbalance, gastrocnemius dysfunction, anatomical variations of the plantaris muscle, poor tendon vascularization, torsion of the Achilles tendon, fascicle slippage, and lateral ankle instability.
Extrinsic factors involve mechanical overload, repetitive stress, use of inadequate or worn-out equipment, obesity, certain medications (such as corticosteroids, anabolic steroids, and fluoroquinolones), improper footwear, insufficient warm-up or stretching, training on hard surfaces, and direct trauma[3].
The incidence of Achilles tendinitis is estimated to be around 7–9% among elite runners, highlighting its significant impact in the field of sports medicine[1].
Pathophysiology of Achilles Tendinitis
The pathophysiology of Achilles tendinitis involves a complex interaction between inflammatory and degenerative processes. In the early stages, repetitive microtrauma to the tendon triggers an acute inflammatory response. Macrophages and neutrophils infiltrate the affected area, releasing pro-inflammatory cytokines such as interleukin-1 beta (IL-1β) and tumor necrosis factor alpha (TNF-α), along with reactive oxygen species, all of which contribute to pain and tissue injury. As the condition becomes chronic, inflammation subsides, giving rise to a degenerative, non- inflammatory phase known as tendinosis. In this stage, inflammatory cells are replaced by fibroblasts and myofibroblasts, leading to an imbalance between extracellular matrix (ECM) synthesis and degradation. Hyperactive tenocytes proliferate excessively, producing disorganized and weakened collagen fibers. The accumulation of proteoglycans and glycosaminoglycans further disrupts the tendon’s structural integrity. Additionally, the upregulation of matrix metalloproteinases (MMPs) and the downregulation of their natural inhibitors, tissue inhibitors of metalloproteinases (TIMPs), accelerate ECM breakdown. Together, these cellular and molecular changes transform a healthy, resilient tendon into one that is structurally compromised, painful, and functionally impaired[1].
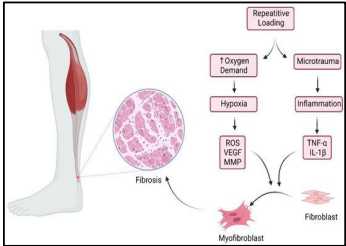
Fig. 1: Pathogenesis of Achilles tendinitis
MATERIALS & METHODS
The study was conducted in the outpatient department of Physical Therapy after obtaining informed consent from the patient. The participant was a 64-year-old male shopkeeper diagnosed clinically with chronic Achilles tendinitis, with symptoms persisting for approximately 8 months prior to intervention. The patient reported posterior ankle pain and morning stiffness, aggravated by prolonged standing and walking during occupational activities. Baseline functional limitation included difficulty in initiating walking in the morning and pain during prolonged weight-bearing. Prior to enrollment, the patient had received intermittent conservative management, including rest and occasional use of oral analgesics, with no structured physiotherapy or exercise-based rehabilitation. Before the intervention, pain intensity was assessed using the Visual Analog Scale (VAS). No objective assessment of tendon strength or functional performance was performed at baseline.
Fig. 2: Site of achilles tendinitis
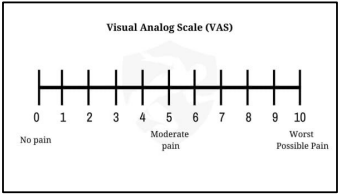
Figure 3: Visual analog scale
Intervention protocol
The treatment consisted of an eccentric loading exercise program targeting the Achilles tendon. Prior to each session, the patient performed a brief warm-up of five minutes, consisting of gentle ankle range-of-motion exercises. No additional stretching exercises were prescribed during the intervention period. The patient was instructed to stand on a step with the forefoot placed on the edge, heels elevated, and knees maintained in extension. From this position, the unaffected leg was lifted, and the affected heel was slowly lowered to the maximum tolerable range and held for 10 seconds. The unaffected leg was then used to assist in returning to the starting position, which was also held for 10 seconds. The exercise was performed for three sets of 15 repetitions, with a one-minute rest interval between sets. The program was carried out once daily, five days per week, for six weeks. The patient was advised to avoid high-impact activities and ensure adequate rest between sessions.
OUTCOME MEASURE
To pain level documentation: visual analog scale
Outcomes were assessed at baseline (pre-treatment) and again after 2, 4, and 6 weeks of treatment. Pain intensity was measured using the Visual Analog Scale (VAS), where 0 indicates “no pain” and 10 indicates “the worst pain imaginable.” Patients were instructed to record their pain level immediately upon waking each morning.
Eccentric Loading Exercise Protocol
Patients were instructed to perform eccentric heel drop exercises on a step. They stood with the forefeet (balls of the toes) positioned on the edge of a step, heels elevated, and knees extended. From this position, the unaffected leg was lifted off the step, and the affected heel was slowly lowered to its maximum range, maintaining the position for 10 seconds. The unaffected leg was then placed back on the step to assist in raising the body to the starting position, which was also held for 10 seconds. This sequence was repeated for three sets of 15 repetitions, with a one-minute rest between sets. The exercise program was performed once daily, five days per week, over a period of six weeks.
RESULT
| Time Point | VAS Score |
|---|---|
| Week 0 (pre- intervention) | 7/10 |
| Week 2 | 5/10 |
| Week 4 | 4/10 |
| Week 6 | 3/10 |
Table 1: Progression of VAS Scores During intervention

Fig. 4: Starting position of eccentric loading exercise
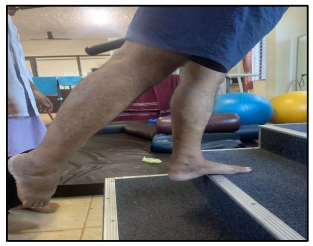
Fig. 5: Controlled raising to end range of ankle planter flexion

Fig. 6: Controlled single-leg lowering in to end range ankle dorsiflexion
DISCUSSION
The purpose of this study is to investigate the effect of eccentric loading exercise on pain reduction and functional improvement in individuals with Achilles tendinitis. Eccentric loading in this study was performed using the heel-drop protocol, which specifically targets the Achilles tendon through controlled lengthening contractions. Pain was assessed using the Visual Analog Scale (VAS), while functional improvement was assessed through clinical observation and reported outcomes. As known, Achilles tendinitis is a common overuse injury, particularly in athletes and individuals engaged in repetitive loading activities, where maintaining tendon strength and flexibility plays a crucial role in performance and injury prevention.
The research conducted by Beyer, et al. (2015) and Prudêncio, et al. (2023)[4] demonstrated that eccentric training significantly reduces pain and improves tendon function, establishing it as an effective first-line management strategy. Similarly, Jayaseelan, et al. (2019)[7] reported that eccentric exercise helps in tendon remodeling and improves dynamic load tolerance. However, studies such as Ranganathan, et al. (2016) and Malliaras, et al. (2018) suggest that while eccentric exercise is beneficial, other protocols like heavy slow resistance (HSR) training may provide comparable or even superior outcomes in certain populations.
Thus, while several studies support the effectiveness of eccentric loading exercise in managing Achilles tendinitis, conflicting evidence exists regarding its superiority over other loading strategies.
As the conclusion remains unclear, further research with larger sample sizes and long-term follow-up is required to determine the most effective rehabilitation protocol for Achilles tendinitis.
CONCLUSION
This study found that the eccentric Loading Exercise in Achilles tendinitis patients gives good prognosis in regards to the pain score which was assessed using VAS, it showed a significant decline in pain score from week 1 to week 6.
DISCLOSURE
Ethical Approval: Approved.
Source of Funding: None.
Conflict of Interest: The authors declare no conflict of interest.
References
1. Jeyaraman N, Jeyaraman M, Ramasubramanian S, Balaji S, Muthu S. Unlocking the Potentials of Exosomes in Achilles Tendinitis. Journal of Foot and Ankle Surgery (Asia Pacific). 2024; 11 (4). Available from: https://doi.org/10.5005/jp-journals-10040-1369
2. Maffulli N, Sharma P, Luscombe KL. Achilles Tendinopathy: Aetiology and Management. Journal of the Royal Society of Medicine. 2004; 97 (10). Available from: https://doi.org/10.1177/0141076809701004
3. Pabón MA, Naqvi U. <I>Achilles tendinopathy</I>. InStatPearls [Internet] 2023 Aug 17. StatPearls Publishing.
4. Prudêncio DA, Maffulli N, Migliorini F, Serafim TT, Nunes LF, Sanada LS, <I>et al</I>. Eccentric exercise is more effective than other exercises in the treatment of mid-portion Achilles tendinopathy: systematic review and meta-analysis. BMC Sports Science, Medicine and Rehabilitation. 2023; 15 (1). Available from: https://doi.org/10.1186/s13102-023-00618-2
5. Ko VM, Cao M, Qiu J, Fong IC, Fu SC, Yung PS, <I>et al</I>. Comparative short-term effectiveness of non-surgical treatments for insertional Achilles tendinopathy: a systematic review and network meta-analysis. BMC Musculoskeletal Disorders. 2023; 24 (1). Available from: https://doi.org/10.1186/s12891-023-06170-x
6. Sivrika AP, Papadamou E, Kypraios G, Lamnisos D, Georgoudis G, Stasinopoulos D. Comparability of the Effectiveness of Different Types of Exercise in the Treatment of Achilles Tendinopathy: A Systematic Review. Healthcare. 2023; 11 (16). Available from: https://doi.org/10.3390/healthcare11162268
7. Jayaseelan DJ, Mischke JJ, Strazzulla RL. Eccentric Exercise for Achilles Tendinopathy: A Narrative Review and Clinical Decision-Making Considerations. Journal of Functional Morphology and Kinesiology. 2019; 4 (2). Available from: https://doi.org/10.3390/jfmk4020034
8. Ryan D, O’Donoghue G, Rio E, Segurado R, O’Sullivan C. The effect of combined Action Observation Therapy with eccentric exercises in the treatment of mid-portion Achilles-tendinopathy: a feasibility pilot randomised controlled trial. BMC Sports Science, Medicine and Rehabilitation. 2022; 14 (1). Available from: https://doi.org/10.1186/s13102-022-00594-z
9. Murphy MC, Travers MJ, Chivers P, Debenham JR, Docking SI, Rio EK, <I>et al</I>. Efficacy of heavy eccentric calf training for treating mid-portion Achilles tendinopathy: a systematic review and meta-analysis. British Journal of Sports Medicine. 2019; 53 (17). Available from: https://doi.org/10.1136/bjsports-2018-099934
10. Mansur NS, Matsunaga FT, Carrazzone OL, Dos Santos BS, Nunes CG, Aoyama BT, <I>et al</I>. Shockwave Therapy Plus Eccentric Exercises Versus Isolated Eccentric Exercises for Achilles Insertional Tendinopathy. Journal of Bone and Joint Surgery. 2021; 103 (14). Available from: https://doi.org/10.2106/jbjs.20.01826
11. Gatz M, Betsch M, Dirrichs T, Schrading S, Tingart M, Michalik R, <I>et al</I>. Eccentric and Isometric Exercises in Achilles Tendinopathy Evaluated by the VISA-A Score and Shear Wave Elastography. Sports Health: A Multidisciplinary Approach. 2020; 12 (4). Available from: https://doi.org/10.1177/1941738119893996
Copyright
© 2026 Published by Laxmi Memorial Education Trust. This is an open-access article under CC BY 4.0 license. (https://creativecommons.org/licenses/by/4.0/)
Cite this article
K Bhoomika, K H Bharath, Shruthi P Puthran. The Effect of Eccentric Loading Exercise in Achilles Tendinitis– A Case Study. AJ J Med Sci 2026;3(1):33-37