
Metastasis to the temporal bone is an infrequent clinical entity, often associated with advanced malignancy. The most commonly implicated primary sites include breast, lung, prostate, and renal carcinomas. Due to its rarity and the non-specific nature of symptoms, temporal bone metastasis is frequently misdiagnosed or overlooked during initial evaluation. Patients may present with signs mimicking benign otologic conditions such as chronic otitis media, facial nerve dysfunction, hearing loss, or vertigo.
Among these, facial nerve palsy, persistent otorrhea, and sensorineural hearing loss are notable indicators but are rarely immediately linked to metastatic disease. Temporal bone involvement as the first clinical sign of an undiagnosed systemic malignancy is particularly uncommon and presents a significant diagnostic challenge.
This case report discusses an unusual presentation of metastatic breast adenocarcinoma manifesting primarily with facial nerve palsy and mimicking a benign otologic disorder, ultimately leading to the diagnosis of advanced systemic malignancy.
A 61-year-old female, known case of rheumatoid arthritis, presented with sudden-onset left-sided lower motor neuron facial palsy of 20 days duration. She also reported a history of intermittent back and joint pain over the preceding months. Initial management included low-dose corticosteroids, which were later escalated to high-dose steroids due to lack of clinical improvement. Despite this, there was no resolution of facial weakness.
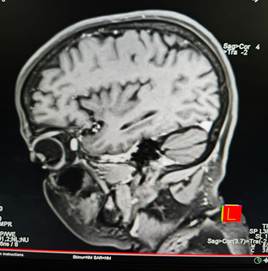
As symptoms persisted, an MRI of the brain and temporal bone was performed, which revealed lytic lesions involving the left mastoid and petrous temporal bone. In view of these findings and the progressive nature of the facial palsy, the patient underwent an emergency mastoid exploration under general anesthesia.
Intraoperatively, a pale pink, friable proliferative mass was found occupying the mastoid cavity, with erosion of the dural plate, ossicles, and facial nerve canal, and extension toward the petrous apex. Complete excision was not feasible due to proximity to critical neurovascular structures; however, maximum debulking was performed. Conchomeatoplasty was carried out, and biopsy specimens were sent for histopathological evaluation. A second-stage surgery was planned for hearing reconstruction.
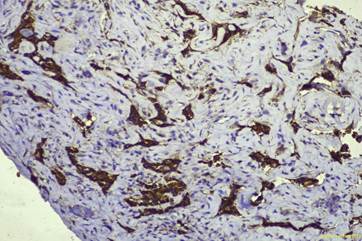
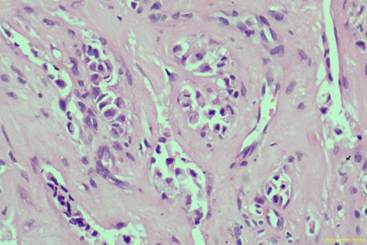
Histopathology revealed a poorly differentiated adenocarcinoma, and immunohistochemistry confirmed it to be of breast origin. Subsequently, a whole-body PET-CT was performed to locate the primary and assess the metastatic burden. The scan showed an FDG-avid, heterogeneously enhancing, lobulated lesion in the retroareolar region of the right breast, measuring 4.4 × 3.4 × 5.1 cm, with central skin infiltration. Additional findings included:
Non-FDG avid satellite nodules surrounding the primary lesion.
FDG-avid cutaneous nodules in the right breast.
Right axillary Level I lymphadenopathy (largest node 1.5 × 1.4 cm).
No significant supraclavicular or internal mammary involvement.
A single faintly FDG-avid pulmonary nodule (7.5 mm, SUVmax 1.3) in the left lung.
Multiple lytic and sclerotic lesions involving the left temporal bone, right mandible, humeral head, scapula, sternum, spine, pelvic bones, and femurs, with the highest FDG uptake (SUVmax 7.4) noted in the left sacral wing.
Temporal bone metastasis is an uncommon but clinically significant manifestation of systemic malignancies. Breast cancer is among the most frequent primary tumors to metastasize to the temporal bone, along with lung, kidney, and prostate carcinomas
In this case, the patient's initial presentation with isolated facial nerve palsy is consistent with prior reports indicating that facial nerve involvement is a common early symptom of temporal bone metastasis
Histologically, metastatic adenocarcinomas are often poorly differentiated, requiring immunohistochemical staining to confirm tissue of origin, as demonstrated in this patient. Literature indicates that breast cancer frequently metastasizes to the petrous apex and internal auditory canal, with erosion of adjacent structures
The differential diagnosis of destructive temporal bone lesions should include primary temporal bone malignancies, metastatic disease, and granulomatous conditions
Surgical intervention in such cases is often limited to biopsy or debulking for diagnostic and palliative purposes, given the proximity to critical neurovascular structures and the disseminated nature of disease. Definitive management typically involves systemic therapy tailored to the primary tumor and extent of metastasis
This case reinforces the need for a high index of suspicion for metastatic disease in patients with atypical or treatment-resistant facial palsy. Early identification and multidisciplinary management are essential to optimize patient outcomes.
Metastatic involvement of the temporal bone is an infrequent clinical finding and is more often identified during post-mortem evaluations in patients with advanced-stage malignancies. Among various primary cancers, breast carcinoma is recognized as the most common source of temporal bone metastasis in female patients. The clinical presentation is typically nonspecific, with symptoms such as facial nerve palsy, chronic ear discharge, hearing loss, and vertigo. These symptoms can closely mimic benign middle ear diseases, often leading to misdiagnosis and delays in appropriate management.
Several reports have highlighted the diagnostic challenges in such cases. In a case by Lee
Yeh
| Lee, | Breast | Facial palsy, otorrhea | Histopathology, PET-CT | Temporal bone metastasis as initial sign of breast carcinoma |
| Chang, | Breast | Otitis media-like symptoms | Imaging, Biopsy | Mimicked chronic otitis media; intraoperative biopsy led to diagnosis |
| Yeh, | Breast | Hearing loss, vertigo, facial palsy | HRCT, Histopathology | Nonspecific otologic symptoms delayed diagnosis |
| Keles, | Breast | Mimicked chronic otitis media | Surgery, Histopathology | Reinforced need for biopsy in atypical otitis media presentations |
| Ianniello, | Various | Skull base pain, cranial neuropathies | MRI, PET-CT | Described imaging features of skull base metastases |
| Saito, | Multiple | Otologic symptoms with known malignancy | Histopathology, IHC | Importance of immunohistochemistry in identifying metastatic adenocarcinoma |
| Lee, | Breast | Systemic metastasis | PET/CT | PET/CT essential in detecting occult primary and bone spread |
| Head Neck Pathol, 2009, 2017 | Breast, Lung, Others | Deafness, otalgia, cranial nerve palsy | Histopathology | Emphasized histologic variants and diagnostic role of tissue biopsy |
Advanced imaging modalities contribute significantly to diagnosis and staging. Ianniello
Given the complex anatomy of the temporal bone and its proximity to critical neurovascular structures, complete surgical excision is often not feasible. However, exploratory surgery and targeted biopsy remain essential when clinical suspicion is high, especially in the presence of cranial nerve deficits or symptoms unresponsive to standard treatment. Prompt histopathological diagnosis enables early systemic evaluation and facilitates initiation of appropriate oncologic management.
Temporal bone metastasis, though rare, should be considered in the differential diagnosis when patients present with atypical or persistent otologic symptoms—especially facial nerve palsy, chronic otorrhea, and hearing loss unresponsive to conventional therapy. This case underscores the diagnostic challenges posed by such presentations and highlights the importance of maintaining a high index of suspicion, even in the absence of a known primary malignancy. Surgical exploration and histopathological evaluation, including immunohistochemistry, are vital for accurate diagnosis.